MULTIPLE SCLEROSIS is aptly named for the scleroses (scars or plaques) that occur as the disease resurfaces in multiple episodes.
Diagnosis of multiple sclerosis – the 2010 update
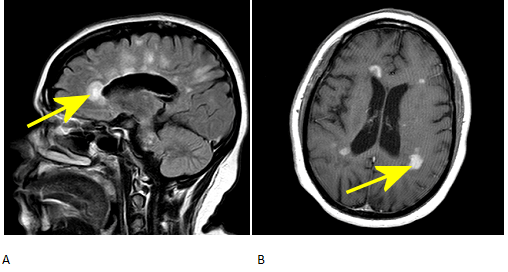
The McDonald Criteria for diagnosing MS was updated in 2010 to help simplify the use of images, and in cases, use one MRI to establish dissemination in space and time and allow for earlier diagnosis. In those criteria, the gold standard remains 2+ attacks = clinical evidence of 2+ lesions = 1 lesion + 1 episode by reliable history, but the presence of both gadolinium-enhancing and non-enhancing lesions on baseline MRI can substitute for a follow-up scan as long as the enhancing lesion is not due to a non-MS pathology. Gad-enhancing lesions in multiple sclerosis represent disease activity usually of up to 6 months; by contrast, T2 lesions represent older, scarred areas. See Figure 1.
Figure 1: A. Dawson’s fingers on sagittal FLAIR image. B. GAD-enhancing lesions on axial T1 image.
Pathophysiology of multiple sclerosis
The immune system attacks the central nervous system. As specific targets of immune attack in MS not identified, MS is an immune-mediated disease. The immune attack damages myelin, which in turn forms scars.
Epidemiology of MS
With the caveat that misdiagnosis is common, worldwide over 2 million people are affected according to the National MS Society as of 2013. As is common in immune-mediated diseases, MS has a 2-fold female predilection. Although can occur in any age, it is usually diagnosed around ages 15-50. Family history and living at northern latitudes are associated risk factors.
Clinical features of MS
Initial symptoms include changes in sensation, strength, vision, gait, dexterity, coordination, balance, and sphincter function. Nonspecific heralding symptoms include malaise, fatigue, and headache. CNS plaques on MRI and lumbar puncture demonstrating oligoclonal bands and increased IgG antibodies are diagnostic.
Clinical Course of MS
Four subtypes of MS have been classified: fortunately, the initial course of most patients with MS is relapsing-remitting. Along with the initial presenting symptoms, patients also suffer from muscle spasticity, pain, as well as urinary and sexual dysfunction. See Figure 2.
No cure for MS exists, however current treatments reduce symptoms and disability.

Figure 2: The clinical course defining four subtypes of multiple sclerosis – progressive-relapsing MS, secondary progressive MS, primary progressive MS, and relapsing-remitting MS
The key immune-mediated disease modifying treatments for relapsing-remitting MS of historical and contemporary relevance include interferons, glatiramer acetate, mitoxantrone, nataluzimab, teriflunomide, fingolimod, and dimethyl fumarate (BG-12). Additional therapies are also currently undergoing clinical trials. Most patients are also on an anti-spasmodic, as well as analgesic for neuropathic pain.
Devic’s disease, also known as Neuromyelitis optica (NMO) as an important variant which consists of simultaneous optic neuritis and myelitis (inflammation and demyelination of the spinal cord). MRI lesions may be found in the spinal cord, but patients can have a normal brain MRI. It is associated with serum aquaporin 4 autoantibodies and poor response to some standard MS treatments.
References:
- Cree AC. “Diagnosis and differential diagnosis of multilple sclerosis.” Continuum Lifelong Learning Neurol. 2010 16 (5): 19-36.
- He et al. “Enhancing Patterns in Multiple Sclerosis: Evolution and Persistence.” AJNR Am J Neuroradiology. 22:664–669, April 2001.
- Heun R, Kappos L, Bittkau S, et al. Magnetic resonance imaging and early diagnosis of MS. Lancet 1988;2:1202–1203.
- Barkhof F, van Walderveen MA, et al. The effect of gadolinium on the sensitivity and specificity of MR in the initial diagnosis of multiple sclerosis. Am J Neuroradiol. 1995;16:259–264.
- Multiple Sclerosis Association of America. “Symptom Management.”
- National Multiple Sclerosis Society. “What is Multiple Sclerosis?”
- Polman et al. “Diagnostic criteria for multiple sclerosis: 2010 Revisions to McDonald Criteria. Annals of Neurology. 69(2) Wiley. pp292-302. 2011.