Multiple Sclerosis expert Dr. Anthony Reder from the University of Chicago Department of neurology is interviewed by Dr. Rui Guan on topics in MS of interest to neurologists and general practitioners alike.
About Dr. Anthony Reder:
Dr. Reder has authored or co-authored over 100 scientific papers on multiple sclerosis, ranging from the basic science of neuro-immunology to therapeutics. He is most well-known for his work on the mechanism of action of interferon in the treatment of MS. He directs the Neurology and Inflammatory Disease Infusion Center at the University of Chicago.
When to refer to an MS specialist?
Dr. Rui Guan: When should a primary doctor refer to a neurologist and when should a general neurologist refer to a multiple sclerosis (MS) specialist?
Dr. Anthony Reder: As of 1993, we finally had a treatment for MS. Interferon-beta required special understanding. Over 20 years, the field has gotten much more complicated, with 9 drugs, with wide spectra of effects and efficacies on relapse, cognition, progression, and lifespan. The initial decision to put people on a therapy often should be with a MS specialist. But once someone is on a drug, it is important for the general neurologist or primary care physician (PCP) to monitor the patient because a lot of other things go wrong or interact with the therapy. For instance, the patient may have high cholesterol or bladder infections. [The generalists] should also be moderately aware of how MS drugs might affect their domain. For example, statins can block interferon action.
RG: You published a paper about statin and interferon interactions in 2012. And this is true with high dose statins. [Arch Neurol. 2012 Oct;69(10):1303-9. Inhibition of interferon-beta responses in multiple sclerosis immune cells associated with high-dose statins.Feng X, Han D, Kilaru BK, Franek BS,Niewold TB,Reder AT.]
AR: Yes, I have a patient who takes interferon at 8am and a statin at 10pm. In another example, Cipro® and Levaquin® can occasionally induce attacks of MS because they are pro-inflammatory—great for infections, not great for MS. I’m not saying every MS patient should be seen by MS specialists all the time, because we just can’t do it. We have a very important partnership with the primary doctors.
MS specialty
RG: What makes a MS specialist?
Dr. Anthony Reder: Knowledge can be accrued as it comes. Fellowship isn’t the only route to being educated in the intricacies of MS diagnosis and management. One can have done the right fellowship, or be a smart, observant, well-read person.
RG: Given so many different drugs, both FDA- approved drugs and others on the horizon, how do you counsel patients who come to you?
AR: It depends on efficacy, risk tolerance, and lifestyle. For example, some people won’t even consider Tysabri® (natalizumab), even if they are antibody negative [for JC virus] because the feel there is still a very remote risk of PML (progressive multifocal leukoencephalopathy). Another occasional hurdle is whether they can do injections? Do they have the right amount of body fat? Are they needle-phobes? Are they fashion models who worry about the slightest changes in their skin? This can be a problem with Copaxone® (glatiramer) and the beta-interferons. Is the patient a lawyer worried about cognitive function? One interesting side-line that we have see here–many of the people who are JCV+ and go on Tysabri® tend to be physicians. Apparently physicians make up a group that doesn’t care about [the risk of] death. I have had 3 [JCV+] doctors who have gone on the drug. It’s an all or nothing approach to life.
RG: Very extreme indeed. When MS patients come to you, what is your philosophy regarding MRIs?
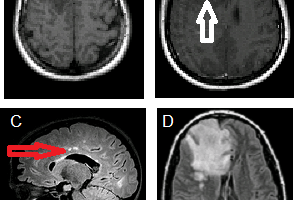
AR: I realize MRIs do give additional information, but the cost of an MRI must be counter balanced with knowledge about how often it will truly inform treatment decisions. If someone is doing worse on a drug, you’re going to change therapy. If someone is stable for many years on every measure possible – her job’s good, there is no fatigue, no cognitive problems, everything in the neurological exam is good, she’s still doing well in her triathlons, and her life has not changed – then the MRI probably doesn’t matter. There are some papers stating that if you have 3 or more new Gadolinium-enhancing lesions in the first year, then patients will not do well on Avonex® (interferon beta-1a). That’s true. But, it’s hard to ferret out any information about how these patients are doing clinically. Did they also have exacerbations that would have prompted them to change drugs?
New drugs and clinical trials for multiple sclerosis
RG: When patients ask about the new compounds coming through the pipeline, how do you counsel them?
Dr. Anthony Reder: Alemtuzumab (Campath®) is coming and seems to be the most effective drug for early MS, but 1/3 patients may develop thyroid disease and other complications. So risk is significant. Laquinomod, had only modest effects on relapses, but did have a stronger effect on stopping progression – out of all of our drugs, that’s the first one in that direction. There are many other drugs in the pipeline, but those are the next in the queue.
RG: How do you counsel patients about clinical trials?
AR: This is an issue. There are many drugs available and it’s overwhelming enough to explain all of the approved drugs. Unfortunately, trial enrollment in the US has plummeted, it’s 1/10 of what it was– the age of big trials in the US is over. Some people do not want to take a placebo or a drug they consider “less effective” when there are so many available approved drugs. There are also people without insurance who would love to be in trials, but they can’t come in the door if they don’t have insurance. If they go into a trial, then there’s a fiduciary obligation to treat them thereafter. So that’s a problem financially for the hospitals involved.
Nonetheless, drugs in development could be more effective or less costly than current treatments, and some people do want to participate in trials. In addition to the 9 FDA-drugs available, I also tell them in clinic that we have some trials that are enrolling patients. One involves an anti-CD19 antibody, similar to Rituxan®, with 4:1 treatment to placebo ratio and could possibly be a very effective drug. Tysabri® and Gilenya® (fingolimod) are being tested for progressive MS.
BAF312 and ONO-4641 are two fingolimod-like molecules under investigation.
Going back to the people with no insurance, they sometimes can’t see specialists in the first place. But, there may be an influx of patients with insurance as Obama Care is phased in. We may see more underserved patients with different disease characteristics and different responses to drugs. In the black population, for instance, there is more CNS Sjogren’s and neuromyelitis optica, and more aggressive MS.
Alternative medicine in MS
RG: What about the role of complementary-alternative medicine in MS?
Dr. Anthony Reder: Around 95% of MS patients are on something in this realm. Especially in the past few years, there has been an increase, and ~90-95% of patients are on vitamin D. The reason is that low vitamin D levels are correlated with development of MS and more frequent MS attacks. Vitamin D with Betaseron® (interferon beta-1b) have an additive effect, resulting in fewer plaques on MRI. MS patients are a very-well informed group, know the vitamin D data, and thus nearly everyone is on vitamin D. Some patients are also on vitamin B12. Evening primrose oil and omega-3 fatty acids suppress inflammation, and are used by a large grup of patients. Equally important is exercise and not being obese, as fat cells secrete pro-inflammatory cytokines.
RG: When giving out tough love, how come the patients have no misgivings about you?
AR: Well, they know they’re wrong [chuckles]. They all know it’s true — especially smoking, which increases attack frequency and doubles the rate of brain atrophy. Of course, some patients do say it’s the last pleasure in life that they have, and I can’t argue with that.
MS Management
RG: Management of MS, especially with changing and starting therapy, should involve an MS specialist – what are some common mistakes when the MS patients come to you?
Dr. Anthony Reder: Something Drs. Arnason, Javed, and Bernard and I see frequently is people who are already on drugs, yet who don’t have MS. It’s very difficult for us to get a patient from a referring doctor who we want to work with [but] has misdiagnosed MS. How do you handle that? The patient is very upset with this news – they just invested everything from joining the support group to getting life insurance. And now they’re on this MS drug [when they actually have] migraine headaches with benign white spots on their MRI. A very dicey situation.
Another [common mistake] is a “zero-tolerance policy” – that the slightest lesion on MRI or slightest change in clinical symptom means you should change to a second, but only partially effective, medicine. It’s a logical fallacy that someone who has done quite well (but not perfectly) on the first drug will do well on another drug. Once you switch drugs, patients may be back to the 1/3 to 50% reduction in relapses. That’s why I said that 3 or more new MRI lesions is a critical threshold, but the logical corollary is that 2 MRI lesions may not matter.
RG: So with a long-term condition like MS, it is important to be sure before diagnosing someone with it.
AR: Yes. And very important for primary physicians to know that if they’re having trouble with the diagnosis, then [the MS specialists] probably will too. Sometimes these cases are not clear cut. We may have to watch for more symptoms, do sequential MRIs to see if there are new lesions, do a spinal tap to confirm that it’s inflammatory, and do evoked potentials if needed. These cases can be complicated, and the patients should be told so.