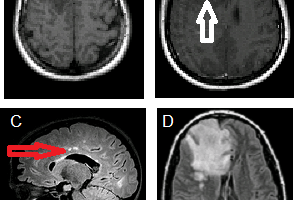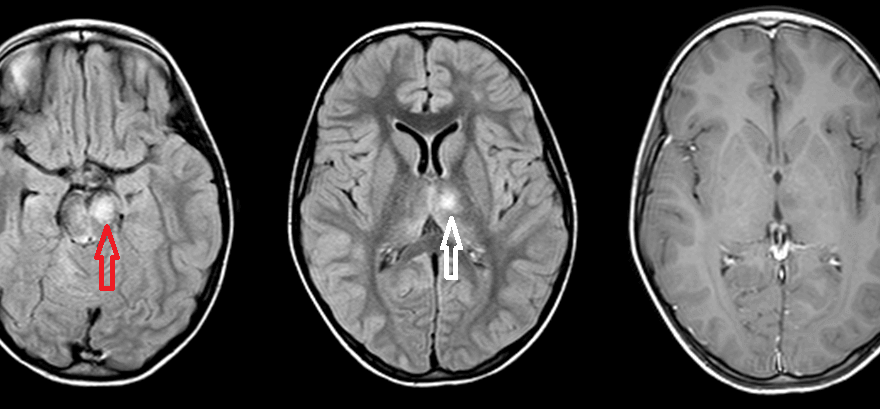
ADEM (acute disseminated encephalomyelitis) is an autoimmune demyelinating disorder distinct from multiple sclerosis or Devic’s disease.

Figure: Axial FLAIR at the level of the midbrain (A) and the thalamus (B) demonstrate increased signal in the left anteromedial thalamus (red arrow) and ventral midbrain (white arrow). Axial postcontrast T1 demonstrates no enhancement of the thalamic signal abnormality (the midbrain abnormality also did not enhance but is not shown).
Discussion:
The vast majority of ADEM cases occur after infection (~95%) or vaccination (~5%), with onset typically between a few days and a few weeks. A variety of infectious agents have been implicated, consistent with an autoimmune basis.
Unlike MS, ADEM does not typically involve the calloseptal interface (the inferior surface of the corpus callosum immediately adjacent to the septum) and it often involves the deep grey matter (thalamus, basal ganglia, dentate etc).
Demographically, ADEM has a slight male predominance (unlike MS) and occurs in a younger age group, typically under 8 years old but any age is possible.
Similar to MS, tumefactive lesions, posterior fossa , subcortical and spinal cord (in about 1/3 of cases) involvement are all possible and lesion signal characteristics are T2/FLAIR hyperintense, variably diffusion restricting and enhancing. Incomplete lesion rim enhancement occurs in both conditions.
ADEM should also be distinguished from posterior reversible encephalopathy syndrome (PRES) and microvascular disease. PRES typically has a posterior predominance with vasogenic edema. Microvascular disease has a different demographic and history and it tends to involve the periventricular white matter, less likely subcotical zones and the posterior fossa. Autoimmune mediated vasculitis can have a similar appearance on brain MRI but CT or conventional angiography will typically reveal intracranial vascular disease.
Hence the combination of suggestive history, right demographic and lesion distribution can be highly suggestive of ADEM. Follow up imaging is helpful in uncertain cases as ADEM is self limiting whereas MS is progressive. Despite its natural history, ADEM is associated with significant neurological morbidity (20-30%, with seizures the most common sequelae) and mortality (10-30%).