An idiopathic palsy of the facial nerve (cranial nerve VII) which results in ipsilateral weakness of the facial muscles.
Clinical Presentation of Bell’s Palsy
Patients present with weakness and sometimes complete paralysis of the facial musculature on the side involved This can manifest as:
- Loss of the nasolabial fold and dropping of the corner of the mouth
- Inability to close the eyes (orbicularis oculi weakness) which can result in corneal exposure and eye irritation from lack of lubrication
- Inability to raise the eyebrow
Symptoms develop acutely over 3-7 days.
Etiology of Bell’s Palsy
Bell’s palsy is believed to result from inflammation of the facial nerve at the level of the geniculate ganglion leading to compression and possible demyelination. The inflammatory process is usually idiopathic though infection with HSV-1 has been postulated by some as the cause.
Differential Diagnosis of Facial Nerve Palsies
- Lyme disease
- Otitis media
- Ramsay Hunt syndrome
- Neurosarcoidosis
- Tumor (cholesteatoma, parotid gland)
- Central nervous system lesions (multiple sclerosis)- these lesions can be differentiated from peripheral etiologies as the forehead muscles are spared in central lesions.
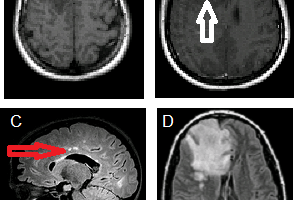
Diagnosis and Work-up of Peripheral Cranial Nerve 7 Palsy
Diagnosis is based on the classical clinical presentation with symptoms occurring acutely over a span of few days. Lyme titers or serology can be checked if history is suggestive. MRI of the brain is indicated to rule out central lesions if the forehead is spared on physical exam.
Treatment
Bell’s palsy usually has a high rate of spontaneous resolution. Though efficacy data is limited, corticosteroids and antivirals have been shown in some studies to improve outcomes
- Corticosteroids: A tapering course of prednisone over 10 days starting at 60 mg/day is recommended.
- Antivirals: Given possible association of Bell’s palsy with HSV-1 infection, antivirals like acyclovir and valacyclovir have been recommended by some. Antivirals seem to work best if prescribed early in the course of onset (within 4 days)
- Eye lubrication: Inability to close the affected eye can lead to corneal ulceration. Eye lubrication should be recommended till the weakness resolves.
Prognosis of Bell’s Palsy
Without treatment, up to 85% of patients show at least partial recovery within 3 weeks of onset. Risk of recurrence after the first episode can be as high as 8%.
Image at http://www.aafp.org/afp/2007/1001/afp20071001p997-f1.gif
References:
Tiemstra, Jeffrey etal. Bell’s Palsy: Diagnosis and Management. Am Fam Physician. 2007 Oct 1;76(7):997-1002