Labyrinthitis is an inflammation of the bony labyrinth that impacts on the function of both the vestibular and auditory systems. Inflammation has a variety of potential causes, and therefore there are mulitple potential etiologies in the differential diagnosis of labyrinthitis.
Presentation of acute labyrinthitis
- Balance problems (vertigo with nystagmus, nausea, dizziness)
- Hearing loss (monaural or binaural)
- Tinnitus (subjective)
- Often preceded by an upper respiratory infection or otitis media
- Nystagmus towards unaffected ear
- Reduced caloric response in affected ear
Viral labyrinthitis
- Hearing loss always present (differentiates from vestibular neuritis)
- 50% of cases follow URI
- Onset acute, lasts days to weeks (residual problems up to months)
- Ramsay-Hunt syndrome
- Herpes zoster infection of labyrinth: Burning pain & vesicular rash of external auditory canal followed by typical symptoms of labyrinthitis
Bacterial labyrinthitis

- Typically secondary to otitis media or meningitis
- Bacterial infection
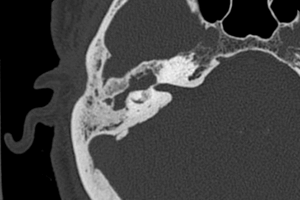
- Suppurative labyrinthitis; usually spread into bony labyrinth from invading cholesteatoma (see cholesteatoma image to the right)
- Inflammatory mediators (bacterial toxins)
- Serous labyrinthitis
- Mediators cross round window membrane and common sequela of otitis media
Autoimmune labyrinthitis
- Uncommon
- Can be either local or secondary to systemic autoimmune disease (eg. Wegener granulomatosis, polyarteritis nodosa)
- Typically bilateral and progressive over weeks to months
- Diagnosis based on clinical response to steroid therapy