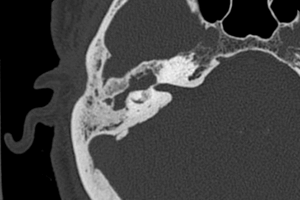
The facial colliculi sit on the dorsal aspect of the pons, forming part of the floor of the fourth ventricle. Both facial colliculi are highlighted in the image below.
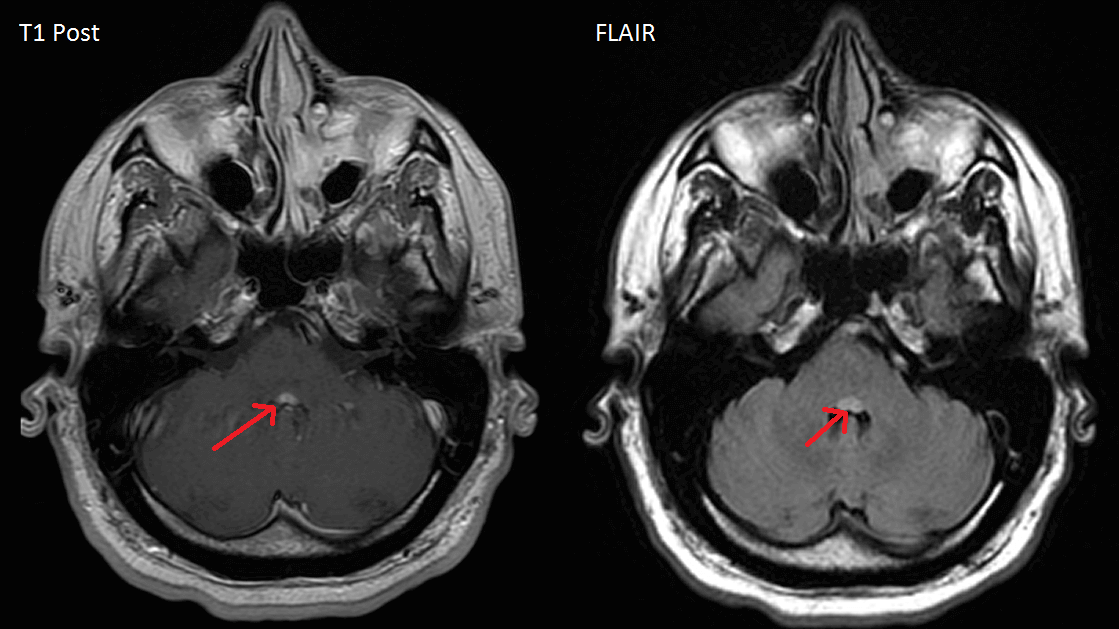
Lesions that affect bilateral facial colliculi are rare, but in the case shown here both are affected by what is likely multiple sclerosis or other demyelinating disease (positive oligoclonal bands and other non-enhancing periventricular white matter lesions). The effects of a lesion are determined by the structures that constitute the facial colliculus, specifically the nucleus of the abducens nerve (CN VI), the facial nerve that wraps around the abducens nucleus, the paramedian pontine reticular formation (PPRF) that sits near the abducens nucleus, and the medial longitudinal fasciculus (MLF).
Facial Nerve Palsy
A lesion of the facial colliculus damages the facial nerve, producing a facial palsy affecting both the top and bottom of the face. This can sometimes be misdiagnosed as a Bell’s palsy, which is also a peripheral VII nerve palsy but by definition is idiopathic. In the case shown above, bilateral facial colliculi lesions would cause bilateral facial weakness.
Ophthalmoplegia
The abducens nerve directly controls abduction in the ipsilateral eye through the lateral rectus. It also controls conjugate adduction of the contralateral eye through the MLF connection to the contralateral oculomotor nucleus. That means that damage to the abducens nucleus would cause loss of abduction of the ipsilateral eye as well as loss of conjugate adduction of the contralateral eye. This is different from lesions of the abducens nerve, which would only cause loss of abduction in the ipsilateral eye.
When both abducens nuclei are lesioned there is a loss of both abduction and adduction in both eyes.
Because the abducens nucleus and the PPRF nearly overlap it is rare to have a lesion of one without the other. However, lesions of just the PPRF can be distinguished from lesions of the abducens nucleus based on the occulcephalic reflex (Doll’s eyes). Because the occulocephalic reflex is mediated by input from the vestibular nuclei to the abducens nuclei, bypassing the PPRF, lesions of just the PPRF will have preserved occulocephalic reflexes. Lesion of the abducens nucleus, with or without lesion of the PPRF, will abolish the doll’s eyes reflex.
Internuclear ophthalmoplegia (INO)
INO is typically the result of lesions of the MLF, since it decouples the contralateral abducens nucleus from the occulomotor nucleus. The typical presentation includes a lack of abduction of the eye on the same side of the MLF lesion. An additional feature is preserved convergence (that is, simultaneous adduction of both eyes), since convergence is not coordinated through the abducens nucleus/MLF pathway onto the oculomotor nucleus.
One-and-a-half syndrome
Unilateral lesions that damage both the abducens nucleus and the ipsilateral MLF (but not the oculomotor nucleus) produce “one-and-a-half syndrome.” These eye movements are characterized by loss of abduction of the eye ipsilateral to the lesion (because of damage to the abducens nucleus), loss of adduction of the contralateral eye (again, because of damage to the same abducens nucleus), and loss of adduction of the eye ipsilateral to the lesion because of loss of input from the contralateral abducens nucleus through the damaged ipsilateral MLF to the ipsilateral oculomotor nucleus. In this case the ipsilateral eye has no medial or lateral movements, while the contralateral eye has no medial (adduction) movement. Again, because the lesion is below the oculomotor nuclei, adduction remains possible with convergent gaze.
Duane’s Retraction Syndrome
Congenital strabismus in which abduction is limited in one or both eyes is called Duane’s Retraction Syndrome. In certain subtypes there is poor development of both the abducens nerve andf the abducens nucleus, which when bilateral can result in lack of abduction or adduction of both eyes.
Two syndrome?
Perhaps non-congenital lesions of both abducens nuclei should be termed “Two Syndrome” since, as in the case shown above, neither eye could adduct or abduct except during convergence when the eyes adducted together. This is consistent with lesions that spares the oculomotor nuclei.
References
de Seze J, Lucas C, Leclerc X, Sahli A, Vermersch P, Leys D. One-and-a-half syndrome in pontine infarcts: MRI correlates. Neuroradiology. 1999 Sep;41(9):666-9.
Kekunnaya R, Gupta A, Sachdeva V, Krishnaiah S, Venkateshwar Rao B, Vashist U, Ray D. Duane retraction syndrome: series of 441 cases. J Pediatr Ophthalmol Strabismus. 2012 May-Jun;49(3):164-9.