Intracranial aneurysms are dilations of the vascular wall. They can be subdivided according to morphology. Fusiform aneurysms are ovoid and elongated, while saccular ones are circumscribed, and spherical. Fusiform aneurysms are less common than saccular ones ; Given their wide neck and elongated morphology, Fusiform aneurysms can be difficult to treat, especially by endovascular methods.
Diagnosis: Fusiform aneurysm
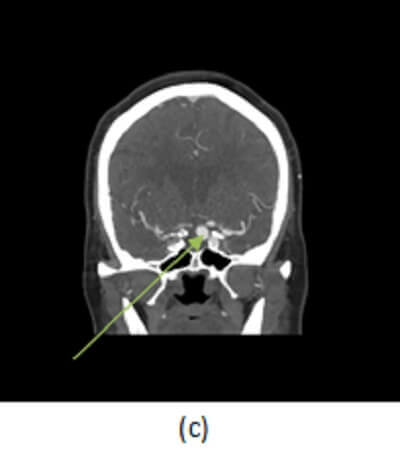
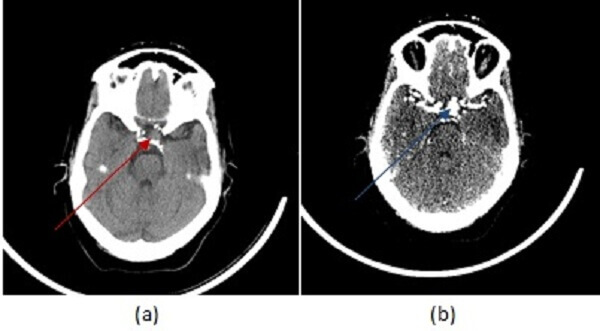
Figure 1: (a, red arrow) non contrast head CT demonstrates a rim calcified mass in the left cavernous sinus projecting towards the suprasellar space. (b, blue arrow) Axial image from a CT angiogram shows vascular enhancement of this mass . These findings are consistent with an aneurysm, likely fusiform. (c) Coronal minimum intensity projection from the CTA shows fusiform dilation of the left cavernous carotid.
Fusiform aneurysms are often due to hypertension and atherosclerotic disease, however they can
also result from dissection or infection (mycotic aneurysms). Dissecting aneurysms result from a tear in the intimal layer of the artery resulting in blood entering the vessel wall and can become pseudoaneurysms if the dissection extends beyond the media layer of the vessel wall. The V4 segment of the vertebral artery is most commonly affected. Mycotic aneurysms tend to be peripheral and bilateral pseudoaneurysms, resulting from destruction of the vessel wall caused by infected emboli, most commonly from bacterial endocarditis.
The risk of aneurysms is rupture leading to subarachnoid hemorrhage and the “worst headache of one’s life”. Symptomatic aneurysms may be coiled or surgically clipped. The procedure selected depends on aneurysm location, morphology and operator experience/preference.