Aphasia is defined as a loss of the ability to understand or produce speech, usually caused by damage to the cerebrum. It is important to clinically classify the type of aphasia a patient has, as this helps localize the lesion and has implications for therapy.
It is first important to distinguish aphasia from dysarthria. Dysarthria is caused by difficulty in the articulation of speech without abnormality in speech comprehension or other linguistic abnormality of speech content. Dysarthria is a mechanical problem (difficulty controlling the mouth musculature to enunciate) rather than a speech content problem.
Etiologies of aphasia
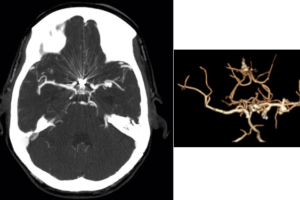
Damage to the cerebrum cause aphasias. The most common cause is ischemic infarction in the dominant hemisphere, especially in the territory of the left middle cerebral artery. Other causes of aphasia include focal intracranial hemorrhages or types of fronto-temporal dementia that affect speech centers.
Classifying aphasias
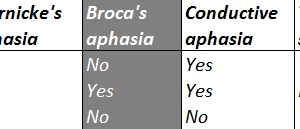
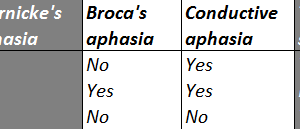
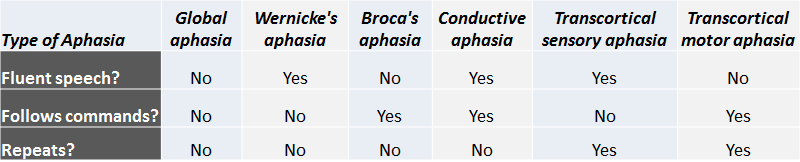
Clinically aphasia can be classified based on a patient’s behavior in response to three questions: 1) is the patient’s speech fluent? 2) does the patient follow commands? 3) can the patient repeat a phrase spoken to him or her?
This chart shows which of six types of aphasia a patient has based on their clinical presentation.
Speech centers
Speech is distributed across the cerebral cortex, usually in the left hemisphere. About 95% of right-handed individuals have the majority of their speech centers in the left hemisphere. 70-80% of left-handed individuals have speech centers in the left hemisphere as well. Speech areas can be re-organized during childhood. For example, young children with tuberous sclerosis and tubers in their left hemisphere reorganize to have more speech centers on the right.
While many cortical areas contribute to speech comprehension and production, two areas are considered central to speech: Wernicke’s area and Broca’s area. The central sulcus separates motor cortex anteriorly from sensory cortex posteriorly. Wernicke’s area is a sensory cortical area is important for speech comprehension. Broca’s area is a motor cortical area and is important for speech production.
Wernicke’s area
Obviously, audition is the primary sensory modality required for speech comprehension. Audition starts in the cochlea, projecting centrally through the 8th cranial nerve to the auditory nuclei of the brainstem, up to the inferior colliculus in the tectum of the midrain, then to the medial geniculate body, and on to the primary auditory cortex in the temporal lobe.
Wernicke’s area sits in the superior temporal gyrus at the posterior edge of the temporal lobe, just next to the parietal lobe, in Brodmann’s area 22.
Lesions of Wernicke’s area causes a type of receptive aphasia known as Wernicke’s aphasia.
Mnemonic: Wernicke’s is for “Wunderstanding.”
Broca’s area
Speech production occurs in the motor areas of the brain, that is, anterior to the central sulcus. The pathway of speech production is not well understood, but Broca’s area is a crucial component.
Broca’s area sits inferiorly in the frontal lobe, just above the anterior pole of the temporal lobe. Broca’s area is made up of the pars opercularis and pars triangularis of the inferior frontal gyrus, Brodmann’s areas 44 and 45.
Lesions of Broca’s area causes a type of expressive aphasia known as Broca’s aphasia.
Mnemonic: Broca’s area is for speech “Broduction.”
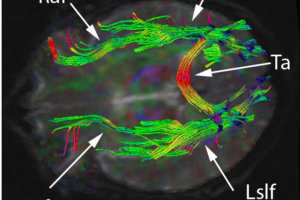
Arcuate fasciculus
Wernicke’s area and Broca’s area are connected with a white matter tract known as the arcuate fasciculus.
In order to repeat phrases that are spoken by others all three structures must be intact. That is repetition requires an intact Wernicke’s area, intact arcuate fasciculus, and intact Broca’s area.
Lesions of the arcuate fasciculus cause a conductive aphasia.
Supporting speech areas
While Wernicke’s area and Broca’s area are the main cortical structures implicated in speech, there are a variety of poorly defined areas surrounding each that influence speech function. Lesions of these areas can cause either an expressive or receptive aphasia, but preserve repetition.
Any aphasia with preserved repetition is considered a “transcortical aphasia.”
Summary of aphasias
In summary, here are the lesions that cause different types of aphasia:
- Lesions of Wernicke’s area cause receptive aphasia.
- Lesions of Broca’s area cause expressive aphasia.
- Lesions of the Arcuate Fasciculus cause conductive aphasia.
- Lesions of supporting areas cause either transcortical sensory or transcortical motor aphasia depending on the location and are characterized by preserved repetition.
- Lesions of the entire left MCA territory cause global aphasia.