Tumors of the pineal gland can be categorized into pineal cell and germ cell depending of their cell type of origin. Unlike germ cell tumors, pineal cell tumors tend to expand the pineal gland with calcifications seen along the periphery of the gland. Unlike non-pineal masses, these primary pineal tumors are much more likely to present with parinaud’s syndrome.
Diagnosis: Pineoblastoma
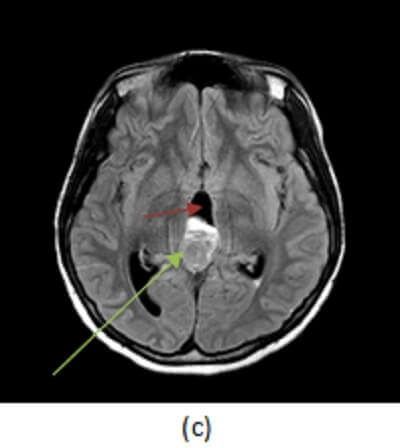
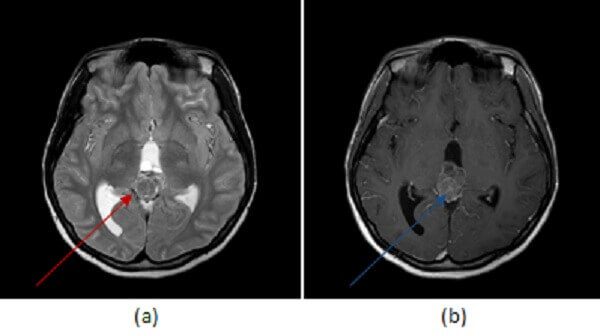
Figure 1: axial T2 (a, red arrow) and FLAIR (b, blue arrow) sequences demonstrate a large lobulated pineal mass with ill defined borders and heterogenous signal. (c, green arrow) post contrast T1 demonstrates heterogenous enhancement to the mass. There is hydrocephalus, manifested by an enlarged third ventricle (purple arrow).
The most common pineal cell tumors include pineoblastoma and pineocytoma.
Pineoblastomas are highly malignant tumors of early childhood, more common in females with peak incidence of 3 years of age. Pineoblastomas are typically large, solid, lobulated masses that compress or infiltrate adjacent structures, that seed the meninges and that may have drop metastasize in the spine. They are heterogenous masses, hyperdense on CT and iso/hypo dense on T2. They enhance heterogeneously and demonstrate restricted diffusion due to high tumor cellularity. Treatment includes surgical resection and radiation of the entire neuraxias (due to the high frequency of metasatasis at presentation).
Pineocytomas are slow growing tumors that may occur at any age but favor young adults. They account for about 45% of pineal cell tumors. Compared to pineoblastomas, they affect an older population, are smaller (typically less than 3 cm), better defined, more homogenous in enhancement and more likely cystic. In fact, the more cystic pineocytomas are indistinguishable from pineal cysts and a diagnostic challenge as both may be stable on serial imaging.