The middle cerebral artery is the major supplier of blood to the cerebral cortex. It consists of 4 principal segments, M1-M4. M1 refers to the horizontal course of the artery from its origin at the supraclinoid internal carotid artery to the sylvian fissure. The M1 segment gives rise to medial and lateral lenticulostriate arteries which supply the lateral thalamus and globus pallidus inferiorly and variably the internal capsule. M1 also gives off the anterior choroidal artery which supplies portions of the hippocampus and posterior limb of the internal capsule.
As the MCA reaches the sylvian fissure, it branches into the anterior temporal artery and in to superior and inferior divisions. The M3 and M4 segments consistent of distal branches of these two divisions, which course over the frontal operculum and supply parts of the frontal, parietal (superior division) and temporal (inferior division) lobes respectively.
Diagnosis: MCA territory infarct
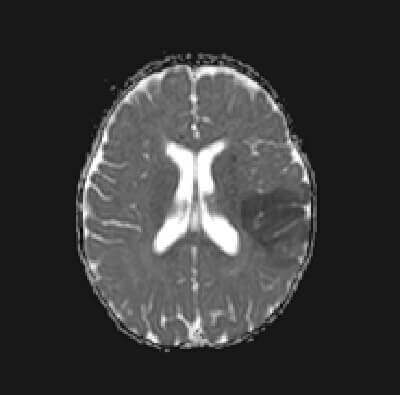
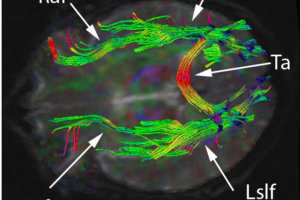
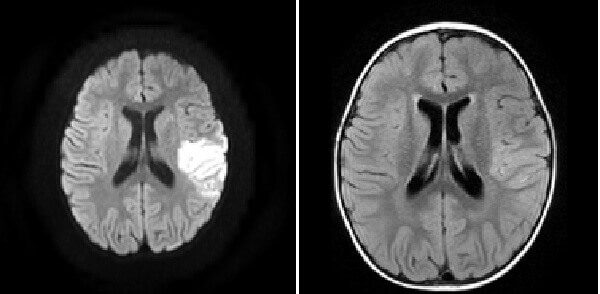
Figure 1: (a, blue arrow) increased DWI signal in the right frontal lobe is also low on ADC
b,red arrow) FLAIR images demonstrate increased cortical signal and sulcal effacement
(c, green arrow) consistent with an acute infarct.
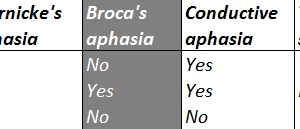
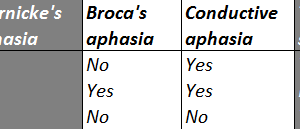
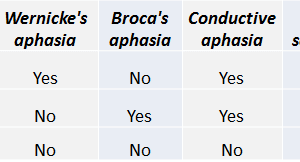
Symptoms of an MCA territory infarct depend on whether the artery supplies dominant language areas, most commonly on the left in right handed individuals. Symptoms of left sided superior division MCA territory infarcts therefore include Broca’s (expressive) aphasia through involvement of the inferior frontal lobe, visual neglect from parietal lobe impairment and contralateral motor and sensory loss preferential for the face and upper extremities (given the distribution of the sensorimotor homunculus in the motor and sensory strips of the pre-and postcentral gyrus). Infarcts of the inferior division include Wernicke’s (receptive) aphasia through involvement of the superior temporal lobe, and partial visual loss especially quadrantanopsia or hemianopsia (as the optic radiations extend from the lateral geniculate to the temporal lobe). Infarcts involving the medial lenticulostriate arteries can present with a dense hemiplegia.