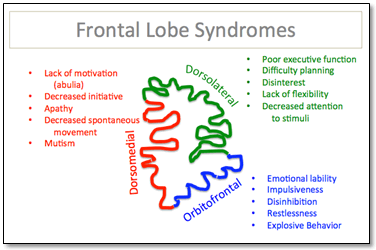
There are three classically characterized syndromes that result from damage to the frontal lobes.
Classic Frontal Lobe Syndromes
Dorsolateral Frontal Lobe Injury
- Function: Monitors and adjusts behavior using ‘working memory’, executive function, planning, strategy formation
- Dysfunction: Lack of ability to plan or to sequence actions or tasks, poor working memory for verbal or spatial information (depending on left versus right cortex), disinterest, decreased attention to stimuli, lack abstract thinking and flexibility in thought, apathy.
Orbitofrontal Injury, Inculding Limbic and Reticular Areas
See example case at the end of the article.
- Function: Emotional input, arousal, suppression of distracting signals.
- Dysfunction: Disinhibition, emotionally labile, memory disorders, impulsiveness, lack of concern for others, distractibility, hyperkinesis, restlessness, explosive behavior.
Dorsomedial Frontal Lobe Injury
- Function: motivation, initiation of action.
- Dysfunction: Apathy, lack of concern, abulia (lack of motivation), decreased awareness and spontaneous movements, may be akinetic or display mutism.
Injury to Other Areas of the Frontal Cortex
- Primary cortex: weakness, tone, impaired fine movements.
- Premotor cortex: proximal muscle weakness (more coarse movements).
- Broca’s area: motor/expressive aphasia on dominant hemisphere, deficits in expressive prosody if non-dominant.
Assessment in Frontal Lobe Injuries
History: In the acute setting history taking requires speaking to family members about a patient’s functional baseline. Specific questions about temperament, emotional lability and judgment.
Specialized Physical Exam Assessments:
Test for abstract thinking, planning, judgement
- Plan and structure activities (ex: How would you bake a cake?)
- Discuss insight into own illness and deficits
- Interpret proverbs
Test for attention and working memory
- Digit span
- Recall
- Copying alternating sequence
- ‘fist-edge-palm’ test
Test language
- Repetition
- Naming
- Word fluency (Name as many words beginning with F in 1 minute as you can)
Check for frontal release signs
- Grasp reflex
- Suck reflex
- Snout reflex
- Palmomental reflex
Formal Testing:
- Wisconsin Card Sorting test: Particularly with dorsolateral lesions, patients perform poorly and have trouble shifting.
- Trail Making: connecting letters and numbers in an alternating pattern.
- Stroop Color and Word Test: reading the names of colors written in a different color.
Differential Diagnosis in Frontal Lobe Injury
- Trauma
- Dementia
- Tumor
- Epilepsy
- Abscess/infection
- Ischemic of hemorrhagic Stroke
- Developmental
Example Case: Bifrontal Contusions
A 32 year old male was brought to the emergency department escorted by police after being found on the ground on an early Sunday morning. He had a large fresh bruise on the back of his head, and had no recollection of what happened. He had no wallet and a high serum alcohol level.
Additional history from his girlfriend suggested the patient was impulsive at baseline and frequently got into fights.
Initial exam showed a well developed, muscular male who was lying quietly, following suggestions passively, and had no focal weakness and had intact speech and comprehension. The patient also complained of loss of taste and smell.
Over the next 3 days he had large swings in mood and at times took aggressive tones to family and hospital staff.
CT head showed bifrontal contusions.

Summary: This is a classic presentation of a traumatic contrecoup injury to bilateral orbitofrontal areas. The change in baseline behavior with emotional lability is often seen with orbitofrontal lesions, and the loss of smell and taste helps with localization.