
It is important to be able to distinguish central from peripheral causes of facial paralysis.
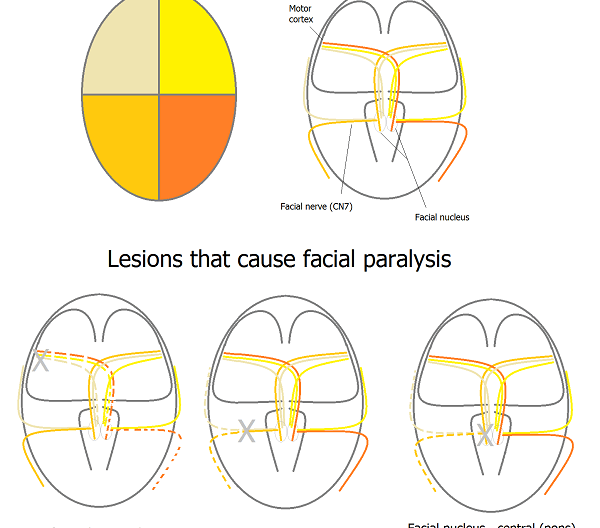
Facial paralysis is caused by lesions in the pathway starting in the motor cortex and ending in the facial nerve (cranial nerve 7). The pathway is shown in the figure below.
Motor cortex sends fibers to the 7th nerve nucleus in the pons. Fibers that control the top part of the face project to both ipsilateral and contralateral facial nerve nuclei, but fibers that control the bottom part of the face only project contralaterally.

As a result, lesions of the motor cortex result in paralysis of the bottom part of the contralateral side of the face. This is the classic “upper motor neuron” lesion of facial paralysis.
Lesions of the facial nerve cause paralysis of the top and bottom part of the face ipsilateral to the lesion. This is the classic “lower motor neuron” lesion of facial paralysis, and produces a facial nerve palsy. The paresis is called a Bell’s Palsy when the etiology for a facial nerve palsy is not known.
Lesions in the pons that damage the facial nucleus or facial colliculus mimic the peripheral nerve lesion in causing paralysis of the top and bottom part of the face ipsilateral to the lesion. However, it is important to distinguish between this brainstem lesion and a facial nerve palsy since expansion of brainstem lesions can have devastating effects on a patient.