Some differential considerations for a partially cystic sellar/suprasellar mass include a cystic macroadenoma, Rathke’s cleft cyst, cranipopharyngioma, aneurysm, arachnoid cyst and epidermoid.
Diagnosis: Craniopharyngioma
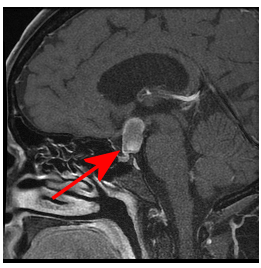
Figure 1A: Sagittal T1 post contast thin section through the midline demonstrates a mass separate from the pituitary (yellow arrow), centered in the suprasellar cistern (red circle).
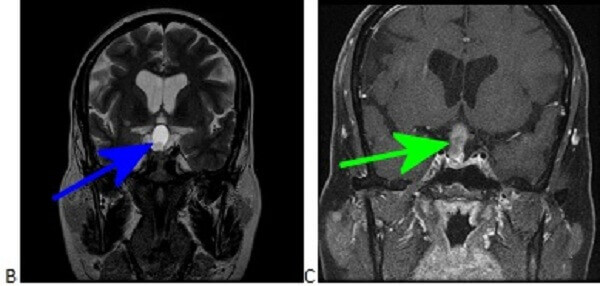
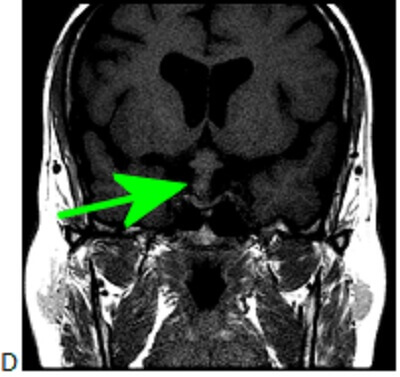
Figure 1B-D: The mass is very T2 hyperintense (B) with a dependent nodule of lower T2 hyperinstensity (blue arrow). Coronal T1 post contrast (C) and pre contrast (D) demonstrate subtle nodular enhancement along the inferolateral margin of the mass (green arrow).
Craniopharnygiomas are neoplasms that originate from the epithelium of the Rathke’s pouch, a depression in the roof of the developing mouth that subsequently develops into the anterior pituitary. Unlike Rathke’s cleft cysts, Craniophranygiomas are typically suprasellar and demonstrate nodular peripheral enhancement and calcification. Craniopharyngiomas most commonly occur in children and in the elderly.