The anterior cerebral artery (ACA) consists of 3 major segments, designated A1-A5 . The A1 segment extends from the middle cerebral artery to the anterior communicating artery (a small artery connecting the contralateral anterior cerebral artery and completing the circle of Willis anteriorly; also the most common location for an aneurysm).
The A1 segment gives rise to medial lenticulostriate arteries that supply the anterior portion of the basal ganglia. In some patients, A1 also gives rise to a recurrent artery of Heubner which supplies the head of the caudate. The A2 segment extends from the anterior communicating artery to the first bifurcation of the anterior cerebral into pericallosal and callosomarginal arteries. The anterior cerebral artery continues posteriorly as the A3 segment formed by the pericallosal artery, which extends into the superior parietal lobe. The callosomarginal artery gives rise to branches supplying the medial frontal lobe and cingulate gyrus. Additional callosal branches form the A4 and A5 segments distally.
Diagnosis: Anterior cerebral artery territory infarct

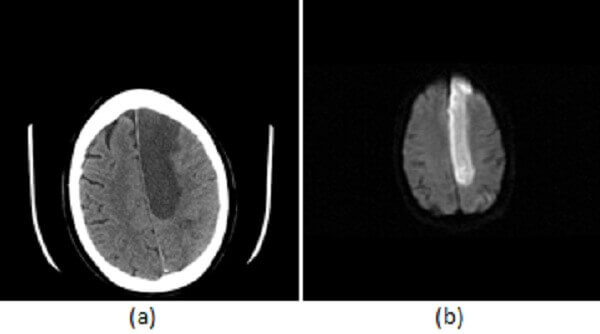
Figure 1: (a) Noncontrast head CT demonstrates hypodensity and mass-effect involving the medial left frontoparietal lobes; (b) Increased restricted diffusion in this territory on DWI consistent with an acute infarct; and (c) MIP reconstructions from an MR angiogram demonstrate major segments of the anterior cerebral artery A1 (red arrow), A2 (blue arrow), A3 (green arrow).
The anterior cerebral artery supplies the gyrus rectus and medial surface of the frontal and parietal lobes, the anterior corpus callosum, anterior portions of the basal ganglia including the caudate head, globus pallidus and anterior limb of the internal capsule.
ACA strokes are less common than those in other vascular territories, accounting for approximately 5% of ischemic strokes. Clinical symptoms of the ACA territory infarct include contralateral leg weakness with sparing of the face (as the ACA supplies the most medial (leg) portion of the sensory homunculus but not more lateral portions like the face). Frontal symptoms including abulia, transcortical motor aphasia (specifically a supplementary motor aphasia) and personality changes due to frontal lobe damage.