Lyme disease is caused by the spirochete, Borrelia burgdorferi. The complete syndrome is actually a manifestation of the infection and the body’s immune reaction to it. The pathogen is transmitted from host to host by the Ixodes or deer tick. The tick is born as a larval tick in the summer and feeds only once, with its preferred host the common field mouse. The following spring the tick becomes a nymph. It again feeds only once. In the fall, the nymph becomes an adult, feeds a single time, but this time with a preferred host being the white-tailed deer.
It requires 2 to 3 days of attachment to an animal before a tick can pass on the infection. This is because infected ticks have only small amounts of bacteria until they feed. Bacteria then multiply in the gut of the tick once feeding begins, and the bacteria migrate to the salivary glands. It is through the salivary gland that the bacteria are injected.
Upon becoming infected, one of three things may happen: patients may handle the infection and never develop symptoms (demonstrated by patients who are asymptomatic but seropositive); B burgdorferi can spread throughout the body and produce symptoms by direct invasion (The inflammatory response to B burgdorferi in the skin probably is the cause of erythema migrans.); B burgdorferi can induce an immune response that may lead to symptoms in various organs, but show no evidence of bacterial invasion.
At present, there is no definitive test for Lyme disease. As pointed out by national guidelines, this means that diagnosis is sometimes difficult. This makes Lyme disease a clinical diagnosis—tests should be used in a supportive role rather than a primary one.
The issue of diagnosis is important because the most important method for preventing chronic Lyme disease is recognition of the early manifestations of the disease and treating them. Early Lyme disease classically presents with a single erythema migrans (EM or “bull’s-eye”) rash. However, the EM rash is present only 50% of the time. A variety of other rashes or no rash at all may occur.
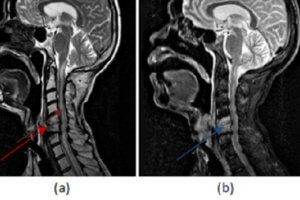
Headache, stiff neck, sleep disturbance, and problems with memory and concentration are findings frequently associated with neurologic Lyme disease. Other less likely neurologic symptoms include numbness and tingling, muscle twitching, photosensitivity, hyperacusis, tinnitus, lightheadedness, and depression.
Chronic Lyme disease is characterized by an indolent onset and variable course. Most patients will have symptoms that are predominantly neurologic and rheumatologic. These symptoms are worse upon awakening. Chronic disease also may produce neuropsychiatric symptoms, and they may be the only manifestation of the disease. Any time a patient presents with musculoskeletal and neuropsychiatric symptoms, chronic Lyme disease should be considered.
Usually, Lyme disease is associated with a paucity of physical findings. However, arthritis, meningitis, and Bell’s palsy may sometimes be noted and should draw attention to Lyme disease as a possibility.
Relative to laboratory testing, even a two-tier diagnostic criteria, using both a positive enzyme- linked immunosorbent assay (ELISA) and western blot, lacks sensitivity and leaves a significant number of individuals with Lyme disease that goes undiagnosed and untreated. These criteria, however, have been designated as rigid diagnostic standards even though they fail to detect up to 90% of cases and do not distinguish between acute, chronic, or resolved infection. In Lyme disease, even CSF evaluation is unreliable for a diagnosis of encephalopathy and neuropathy.
Additional tests for Lyme disease have been evaluated, but the tests have advantages and disadvantages and are yet to be standardized. They remain primarily an option to identify people at high risk for persistent, recurrent, and refractory Lyme disease.
The differential diagnosis of Lyme disease includes thyroid disease, degenerative arthritis, metabolic disorders (vitamin B12 deficiency, diabetes), heavy metal toxicity, vasculitis, primary psychiatric disorders, fibromyalgia and chronic fatigue syndrome.