There was a time when acute mastoiditis was the most common complication of otitis media (AOM). With the advent of antibiotics, this complication has become relatively rare. It is of interest that at a time when the use of antibiotics for all cases of otitis media is being questioned, the members of the ENT community most vigorously questioning this philosophy are those old enough to have encountered mastoiditis on a regular basis. It is still common in underdeveloped countries.
Mastoiditis can be been classified as classic and latent. Classic mastoiditis refers to acute disease following AOM. Latent mastoiditis is also called masked mastoiditis and refers to chronic, subclinical disease that is often secondary to partial treatment of AOM with antibiotics.
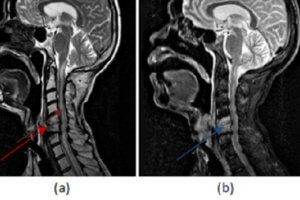
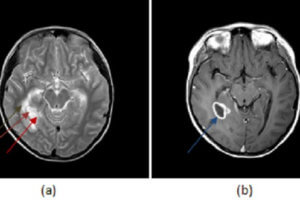
The mechanism of infection is a spread of middle ear inflammation into mastoid air cells, resulting in infection and destruction of the mastoid bone. If inflammation extends through the antrum, it can move into the posterior cranial fossa, the middle cranial fossa, the canal of the facial nerve, the sigmoid and lateral sinuses, and the petrous tip of the temporal bone. Thus the extension of local disease can cause significant morbidity and life-threatening disease.
The bacteriology of acute mastoiditis differs from that of acute otitis media. Acute otitis media is usually caused by S Pneumo or H Flu. Acute mastoiditis is more commonly due to Group A Beta- Hemolytic Strep and S Pneumo with rare involvement by H. Flu. Subacute and chronic diseases usually involve S. Aureus and gram negative rods such as E. Coli, Proteus and Pseudomonas.
The duration of symptoms is what primarily distinguishes mastoiditis from severe acute suppurative otitis media. Otherwise, their signs and symptoms are very similar. Several weeks of the persistent or recurrent symptoms of otorrhea and otalgia suggest development of a coalescent process within the mastoid. A subperiosteal abscess characterized by a fluctuant, inflamed, edematous mass that produces displacement of the ear downward, outward, and forward can develop. The tympanic membrane can simply appear normal, thickened or can demonstrate a small central perforation. Careful attention must be given to the possibility of neurologic changes.
Lab studies should a CBC with differential, ESR, blood cultures, and possibly myringotomy fluid. Plain films are usually inaccurate and delayed with regard to active disease. CT scanning and MRI scanning are of more assistance, particularly if there is any sign of central involvement.
If conservative treatment fails, a mastoidectomy must be considered. There are basically three types of mastoidectomies—simple, radical, and modified radical. The simple, done through the ear, is the preferred.