Vitamin B12, also known as cobalamin, plays an important role in a number of physiological functions, Its deficiency has been associated with macrocytic anemia and number of neuropsychiatric disorders. Further, at the present time, B12 deficiency is being explored with relation to hyperhomocysteinemia and promotion of atherosclerosis.
Measurement of serum vitamin B12 levels is now used to diagnosis vitamin B12 deficiency, but confusing that issue is the fact that 50 percent of patients with subclinical disease have normal B 12 levels. It is now felt that a more sensitive method of screening for vitamin B12 deficiency is measurement of serum methylmalonic acid and homocysteine levels. These are increased early in vitamin B12 deficiency.
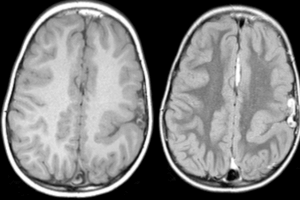
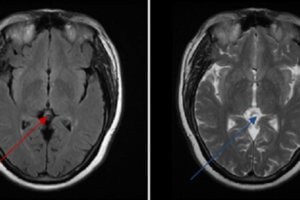
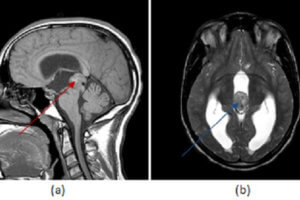
Neurologic symptoms associated with vitamin B12 deficiency include paresthesias, peripheral neuropathy, and demyelination of the corticospinal tract and dorsal columns—also known as subacute combined systems disease—impaired memory, irritability, depression, dementia and, rarely, psychosis. Hematologic manifestations include macrocytic—megaloblastic—anemia and a more advanced stage pancytopenia.
It is now recognized that vitamin B12 deficiency may have indirect cardiovascular effects. In a manner similar to folic acid deficiency, vitamin B12 deficiency can produce hyperhomocysteinemia. This is an independent risk factor for atherosclerotic disease.
The specific symptoms and physical findings with which patients present can be varied because of the wide spectrum of affected systems. These can include typical complaints of aging, such as fatigue, weakness, loss of memory, and depression, but when these symptoms occur in the elderly, vitamin B12 deficiency should be ruled out. Nitrous oxide anesthesia inactivates marginal B 12 stores, and this may exacerbate a process that was subclinical. Shooting pains in the extremities, Lhermitte’s sign, indicate spinal cord involvement, root involvement, or both. While these are not specific for vitamin B12 deficiency, they must raise it as a possibility. Ataxia, altered tendon reflexes, Romberg’s sign, and extensor plantar reflexes are signs of subacute combined systems disease.
Because there are interactions between all the players in the B12, folate, methylmalnomic, homocysteine complex, it is best to use an algorithm for B12 deficiency. This begins with identifying patients at risk, testing for B12 and folate, administering folate if there are low levels, and progressing through a logical sequence.
Neurologic symptoms often improve rapidly with treatment. Damaged nerves may even regenerate. However, the window of opportunity to initiate treatment to reverse or minimize complications is narrow, and it is incumbent upon a clinician to pursue this in the initial workup of patients with dementia and psychiatric disorders.
Likewise, pernicious anemia responds to treatment, but its presentation is often delayed to a time when transfusions are needed to stabilize patients and the pancytopenia ends up being evaluated as a blood dyscrasia.
At one time, it was felt that all patients required parenteral administration of B12 because of malabsorption. This was the basis for a ubiquitous use of B12 shots as treatment for just about any vague complaint. Now, however, there is reasonable evidence that oral treatment will suffice—although this mode of treatment is by no means universally accepted.