Headaches may accompany a variety of conditions of the head or neck.
- Acute—acute onset headache different in character from previous headaches is a medical emergency. Differential contains elements that must all be addressed in a prompt, appropriate manner.
- Vascular bleed (brain aneurysm)—presents with an acute, severe headache, a stiff neck, but no fever. Sometimes, patient has a positive family history of intracranial aneurysm.
- Encephalitis—presents with a headache that is usually constant of increasing intensity and altered sensorium. Increased risk factor is a regional history of viral encephalitis—i.e., Western Equine Encephalitis, West Nile Virus, or Colorado Tick Fever.
- Meningitis—presents with severe headache, stiff neck, and fever. Antecedent history of URI type symptoms or sinusitis may be associated risk factors.
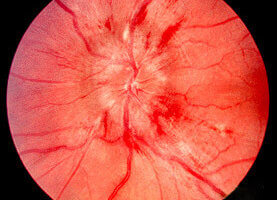
- Temporal arteritis—presents with a headache that is typically throbbing, tenderness over the course of the temporal artery, pain in the masseter muscles, a history of an antecedent illness characterized by malaise and increasing weakness, particularly in proximal muscles, and an erythrocyte sedimentation rate 60 or higher. Represents a medical emergency because if steroid treatment is not quickly initiated, there is a significant incidence of retinal artery thrombosis.
- Tumor (brain tumor)—presents with headache that is of moderate but increasing intensity, often intermittent. Becomes a medical emergency if pressure from tumor begins to cause midline shift of structures.
- Glaucoma—sudden increase in intraocular pressure can cause headache and represents an emergency because of the possibility of retinal damage.
- Cough—Headache that is exacerbated by coughing can be associated with congenital abnormalities such as a Chiari malformation. Acuteness of the headache is typically associated with the acuteness of the cough, but there is roughly a 25% incidence of significant intracranial structural abnormalities associated with this kind of headache.
- New onset vascular (migraine, cluster) headaches—The initial presentation of a cluster headache or even a common migraine may be a dramatic event even though it is not a medical emergency. Cluster headaches are often associated with unilateral rhinorrhea and eye watering.
- Lumbar tap headache—Leakage of spinal fluid following any procedure that involves a lumbar puncture, e.g. epidural anesthesia, can produce a severe headache that can present for up to three days after the procedure.
- Systemic illness—Any febrile illness, infectious disease, particularly mononucleosis, or exacerbation of collagen vascular diseases such as systemic lupus, can cause acute, severe headaches.
- “Computer headache”—Patients can develop severe headaches from unusually long periods spent using a computer, e.g. during the completion of a project with an immanent deadline. The headache is triggered by a combination of eye strain and head and neck muscular spasm.
- Sinusitis (sinus headache)—Acute sinusitis can be associated with severe headaches. Percussion of sinuses precipitates the pain. Fever may also be present. Because of association with sepsis, meningitis, and cavernous vein thrombosis, must be treated aggressively.
- Chronic
- Tension headaches, stress headaches—most common and most chronic form of headache. The only type of headache that can literally last for days. Pain is across the entire head and is often described as a tight band.
- Migraine headaches, cluster headache—presents as intermittent headaches, often triggered by foods, allergies. May actually be the most common type of childhood headache.
- TMJ pain (bruxing, teeth grinding)—frequently overlooked source of chronic and intermittently intense headache. Associated with bruxism which itself may be associated with not only stress but also even mild misalignment of the jaw joint.
- Chronic sinusitis, chronic sinus headache—Plugged sinus ostia can cause sinuses to undergo increase in barometric pressure in a phenomena similar to middle ear not clearing. Pain can be unrelenting. Also associated with trigger for muscular headaches (tension headaches) as well as vascular, migraine headaches. Chronic purulent sinusitis may cause positional pain.